Powered By



 Continue with Facebook
Continue with your email
Continue with Facebook
Continue with your email
When you think of bladder cancer, you most likely have urothelial carcinoma in mind. As the most common type of bladder cancer, urothelial carcinoma accounts for about 90 percent of all bladder cancers.
This article reviews urothelial carcinoma, its symptoms, and its treatment. It also discusses ways to manage the side effects of urothelial carcinoma treatment.
Urothelial carcinoma occurs when urothelial cells that line the inside of the urinary tract begin to grow out of control. Urothelial cells are also known as transitional cells because they transition (change) their shape to stretch when the bladder is full and contract when it’s empty. This is why urothelial carcinoma used to be called transitional cell carcinoma.
Urothelial cells line the entire urinary system, including your kidneys, ureters (the tubes that connect your kidneys to your bladder), bladder, and urethra (the tube that allows you to empty your bladder). Urinary carcinoma can develop anywhere urothelial cells are found. For example, urothelial carcinoma can cause kidney cancer, but this is less common. About 7 percent of kidney cancers are urothelial carcinoma.
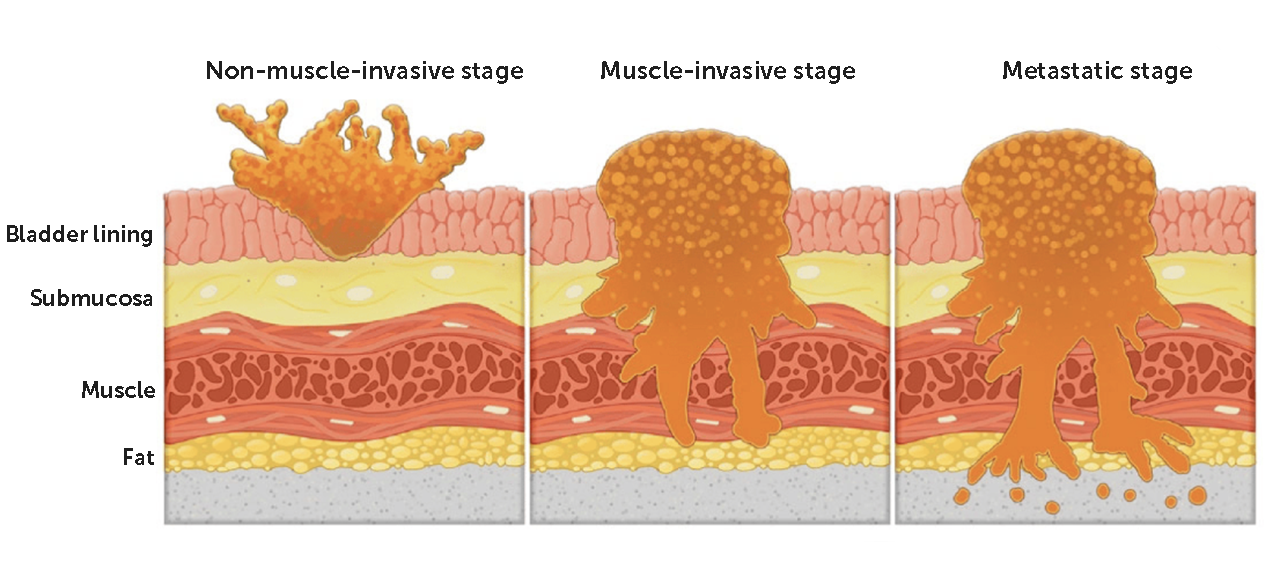
Urothelial carcinoma starts growing in the bladder’s innermost layer. When this occurs, it’s called non-muscle-invasive bladder cancer (NMIBC). NMIBC can also be described as flat or papillary. The term “noninvasive flat carcinoma” refers to when cancer cells grow in a flat patch. “Noninvasive papillary carcinoma” describes a tumor that grows toward the center of the bladder, like a finger.
Noninvasive papillary carcinomas can also be grouped into subtypes based on their appearance under the microscope. This is also called tumor grading.
Low-grade tumors are usually slow-growing and less likely to invade deeper bladder tissues. Noninvasive low-grade papillary urothelial carcinoma is an example of a low-grade urothelial carcinoma. Noninvasive high-grade papillary urothelial carcinoma is a high-grade type that’s more likely to reach deeper tissues.
As cancer cells grow and divide, they can invade deeper bladder layers, such as muscle. If this occurs, it’s called invasive urothelial carcinoma or muscle-invasive bladder cancer (MIBC).
The symptoms of urothelial carcinoma are the same as those of other types of bladder cancer, including:
In the early stages of bladder cancer, when urothelial carcinoma hasn’t become invasive, you may not have any noticeable symptoms. Although most people with bladder cancer will have blood in their urine, the amount may be too small to see or may come and go.
If you have urothelial carcinoma in another part of your urinary tract, such as your kidneys or ureters, you may experience additional symptoms like lower back pain or trouble urinating.
Other medical conditions, such as urinary tract infections, an enlarged prostate, and bladder or kidney stones, can also cause these common symptoms of bladder cancer. This overlap can make urothelial carcinoma difficult to diagnose.
If urothelial carcinoma isn’t caught early, it can continue to grow and cause additional symptoms. Symptoms of advanced, or metastatic, urothelial carcinoma may include:
A pelvic mass (an abnormal growth that starts in the lower abdomen or pelvis) can also be a sign of urothelial cancer.
The process of getting a urothelial cancer diagnosis often starts with a primary care provider. They may suspect urothelial carcinoma because of your symptoms or an abnormal urinalysis (urine test) during a routine exam. If your primary care provider thinks you may have bladder cancer, they’ll refer you to a urologist (a doctor who specializes in treating conditions of the urinary tract and male reproductive organs).
To help diagnose urothelial carcinoma, a urologist may order additional tests such as:
The bladder tissue samples taken during a cystoscopy or TURBT are tested to determine the stage and subtype of urothelial carcinoma. These details can help your cancer care team understand your outlook and the best treatment options for you.
Urothelial carcinoma has also been linked to a family cancer syndrome called Lynch syndrome. Your cancer care team may recommend genetic testing to find out if you have Lynch syndrome. It’s important to know if you have this condition because it also increases your risk of several other cancers, including colon cancer.
Learn more about how bladder cancer is diagnosed.
Treatment recommendations for bladder cancer are generally based on urothelial carcinoma because it’s the most common type of bladder cancer.
The best treatment option for you depends on the type, grade, and stage of your bladder cancer. Your overall health and personal preferences are also important factors when considering bladder cancer treatment.
Surgery is often the primary treatment for bladder cancer. In early-stage urothelial carcinoma, a TURBT may be all that’s needed to remove the tumor. For a high-grade tumor that doesn’t respond to treatments such as immunotherapy, a partial cystectomy (removing part of the bladder) or radical cystectomy (removing the entire bladder) might be done. Doctors usually try less invasive therapies first before recommending a radical cystectomy.
If your whole bladder is removed, you’ll also need reconstructive surgery to create a new way for your body to store and pass urine. This procedure is called urostomy or urinary diversion. Your health care team will teach you how to care for it and adjust to these changes.
Radiation therapy uses high-powered radiation to kill cancer cells. Doctors may recommend radiation therapy to treat urothelial carcinoma when the bladder isn’t removed. This treatment can also be used along with others, such as chemotherapy.
Radiation therapy can cause side effects such as:
Your cancer care team can help you manage side effects. Their suggestions may include the following tips:
Medication may be given before, after, or instead of surgery to reduce the risk of urothelial carcinoma coming back. Drugs used to treat bladder cancer include chemotherapy, immunotherapy, and targeted therapy.
Some chemotherapy and immunotherapy drugs can be placed directly into the bladder, a method known as intravesical therapy. This approach is often used after a TURBT or to treat NMIBC. For NMIBC, this treatment may be given regularly for six weeks to three years, depending on your care plan.
People with MIBC and advanced bladder cancer may need systemic therapy — treatments that work throughout the entire body to kill cancer cells. These systemic medications are injected into a vein or muscle or taken as a pill.
Potential side effects depend on the type of medication. Common side effects may include:
Although medication side effects can be uncomfortable, you can take steps such as these to help manage them:
It’s important to be open and honest with your cancer care team about any new or unusual side effects so they can help you manage them.
If found early, urothelial carcinoma has a good outlook. However, this type of cancer has a high risk of recurring (coming back) after treatment. About 20 percent of early-stage cases might reappear in another part of the body. The risk of recurrence is about 50 percent for stage 2 and 70 percent for stage 3. Most people with stage 4 urothelial carcinoma can’t be cured, but treatment can help manage symptoms and improve quality of life.
Your cancer care team can give you more information about your outlook based on your cancer stage, how you respond to treatment, and your overall health.
MyBladderCancerTeam is the social network for people with bladder cancer and their loved ones. On MyBladderCancerTeam, members come together to ask questions, give advice, and share their stories with others who understand life with bladder cancer.
Have you or a loved one been diagnosed with urothelial carcinoma? What symptoms have you experienced? Share your thoughts in the comments below, or start a conversation by posting on your Activities page.
Get updates directly to your inbox.





 Continue with Facebook
Continue with your email
Continue with Facebook
Continue with your email
Become a member to get even more




 Join
Join
This is a member-feature!
Sign up for free to view article comments.
My thoughts? I wish I hadn't read it this time of night. Now I am more worried about my outcome. Right now, I feel no pain at all. Urinating can be rough if i forget to take my Flowmax. Damn, I don't… read more
We'd love to hear from you! Please share your name and email to post and read comments.
You'll also get the latest articles directly to your inbox.